Abstract: This article provides an in-depth review of the differential diagnosis of dermatitis, emphasizing the various clinical presentations, pathophysiological mechanisms, and diagnostic strategies. The focus is on equipping clinicians with the knowledge to distinguish between the myriad forms of dermatitis.
1. Introduction: Dermatitis, characterized by inflamed, itchy, and often reddened skin, encompasses a range of skin conditions. Effective diagnosis is contingent upon a thorough understanding of the subtle differences between these conditions.
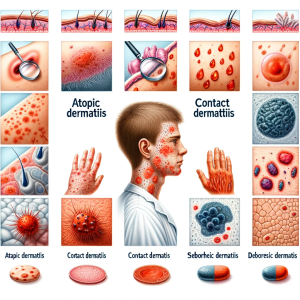
2. Pathophysiological Overview: The pathogenesis of dermatitis varies based on the type. Atopic dermatitis is often associated with a history of allergies and a defective skin barrier. Contact dermatitis, both irritant and allergic, results from skin exposure to offending agents. Seborrheic dermatitis is linked to an inflammatory reaction to Malassezia species.
3. Clinical Spectrum: Each dermatitis subtype presents distinct clinical features. Atopic dermatitis typically manifests as pruritic, eczematous lesions in typical distributions. Contact dermatitis presents acutely with erythema and vesiculation at the site of contact. Seborrheic dermatitis is characterized by greasy scaling over red skin, predominantly in sebum-rich areas.
4. Differential Diagnosis:
4.1 Atopic Dermatitis: Differential diagnosis includes scabies, psoriasis, and other forms of eczema. Key distinguishing features are the chronic, relapsing nature and typical distribution (flexural eczema).
4.2 Contact Dermatitis: Differentiating between irritant and allergic contact dermatitis is critical. Irritant dermatitis is more common, presenting immediately post-exposure, while allergic dermatitis has a delayed onset. Patch testing can be diagnostic.
4.3 Seborrheic Dermatitis: This condition must be differentiated from psoriasis, rosacea, and HIV-associated dermatitis. The distribution and the nature of the scales (oily versus dry) are diagnostic clues.
5. Diagnostic Approaches: Diagnosis of dermatitis is primarily clinical, supplemented by history and physical examination. Skin biopsy, patch testing, and laboratory investigations, including IgE levels and skin swabs, assist in specific scenarios.
6. Therapeutic Implications: Management varies by subtype and includes topical corticosteroids, immunomodulators, and antifungal agents. Addressing the underlying cause, particularly in contact and seborrheic dermatitis, is fundamental.
7. Conclusion: Distinguishing between different types of dermatitis is imperative for appropriate management. A detailed patient history and clinical examination remain the cornerstones of diagnosis, supplemented by targeted investigations.